Compared To Skeletal Muscle Cardiac Muscle Quizlet
Breaking News Today
Mar 18, 2025 · 6 min read
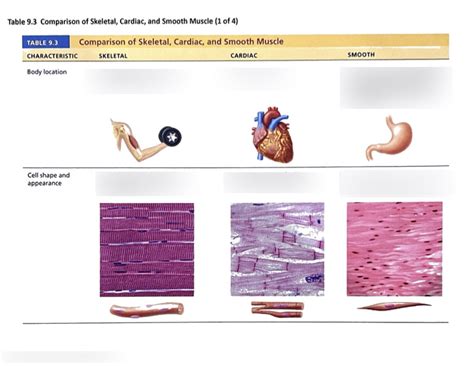
Table of Contents
Cardiac Muscle Compared to Skeletal Muscle: A Comprehensive Overview
Cardiac muscle and skeletal muscle, while both crucial for movement within the body, differ significantly in their structure, function, and control mechanisms. Understanding these differences is fundamental to comprehending the physiology of the cardiovascular system and the musculoskeletal system. This article provides a detailed comparison of cardiac and skeletal muscle, covering key aspects often explored in quizzes and examinations.
Structural Differences: A Microscopic View
The most obvious distinction lies in their microscopic structure. While both are striated, indicating the presence of organized sarcomeres (the contractile units of muscle), the arrangement and composition of these sarcomeres, as well as the overall cell structure, differ substantially.
1. Cell Shape and Size: Skeletal muscle fibers are long, cylindrical, and multinucleated, meaning each fiber contains multiple nuclei located peripherally (near the cell membrane). In contrast, cardiac muscle cells (cardiomyocytes) are shorter, branched, and uninucleated, with the single nucleus centrally located. This branched structure allows for complex three-dimensional networks within the heart, facilitating synchronized contractions.
2. Intercalated Discs: A defining feature of cardiac muscle is the presence of intercalated discs. These specialized structures are not found in skeletal muscle. Intercalated discs are complex junctions that connect adjacent cardiomyocytes, both mechanically and electrically. They contain:
- Desmosomes: These provide strong mechanical adhesion, preventing cells from separating during contraction.
- Gap junctions: These are crucial for electrical communication. They allow for the rapid spread of action potentials (electrical signals) between cardiomyocytes, ensuring coordinated contraction of the heart muscle. This coordinated contraction is essential for effective pumping of blood.
3. Sarcomere Organization: While both muscle types exhibit striations due to the organized arrangement of actin and myosin filaments within sarcomeres, the precise arrangement and the ratio of these filaments might show subtle variations. These variations can influence the force generation and contraction speed.
4. T-tubules and Sarcoplasmic Reticulum: Both muscle types possess a system of T-tubules (invaginations of the sarcolemma, the muscle cell membrane) and the sarcoplasmic reticulum (SR), a specialized internal membrane system involved in calcium storage and release. However, the distribution and density of T-tubules and the extent of the SR differ between cardiac and skeletal muscle. Cardiac muscle has larger and less frequent T-tubules compared to skeletal muscle. The SR in cardiac muscle is less developed than in skeletal muscle, implying a greater reliance on extracellular calcium for excitation-contraction coupling.
Functional Differences: Contraction and Control
The functional differences between cardiac and skeletal muscle are as significant as their structural differences.
1. Contraction Mechanism: Both cardiac and skeletal muscle contraction involves the sliding filament mechanism, where actin and myosin filaments interact to generate force. However, the process of excitation-contraction coupling (the link between electrical excitation and mechanical contraction) differs considerably.
-
Skeletal Muscle: Contraction is initiated by the arrival of a nerve impulse at the neuromuscular junction. This impulse triggers the release of acetylcholine, which leads to depolarization of the muscle fiber and the subsequent release of calcium from the SR. This calcium initiates the cross-bridge cycling between actin and myosin, leading to muscle contraction. The process is largely dependent on the nervous system.
-
Cardiac Muscle: Cardiac muscle contraction is myogenic, meaning it is initiated within the heart muscle itself, primarily by the sinoatrial (SA) node, the heart's natural pacemaker. The electrical impulse generated by the SA node spreads through the heart via specialized conducting pathways, leading to coordinated contraction. While the autonomic nervous system (sympathetic and parasympathetic) can modulate the heart rate and contractility, it does not initiate contraction. Calcium influx from the extracellular space plays a more crucial role in cardiac muscle contraction compared to skeletal muscle. This makes cardiac muscle more sensitive to changes in extracellular calcium levels.
2. Control Mechanisms: The control mechanisms for cardiac and skeletal muscle are vastly different.
-
Skeletal Muscle: Skeletal muscle contraction is under voluntary control, meaning it can be consciously initiated and controlled by the central nervous system.
-
Cardiac Muscle: Cardiac muscle contraction is involuntary and largely regulated by the autonomic nervous system. The sympathetic nervous system increases heart rate and contractility (positive inotropic effect), while the parasympathetic nervous system decreases heart rate (negative chronotropic effect). Hormones such as adrenaline (epinephrine) and noradrenaline (norepinephrine) can also influence cardiac muscle contraction.
3. Fatigue Resistance: Cardiac muscle exhibits a remarkably high degree of fatigue resistance. It can contract rhythmically for a lifetime without significant fatigue. This is in contrast to skeletal muscle, which can fatigue relatively quickly, particularly during prolonged or intense activity. The high fatigue resistance of cardiac muscle is attributed to several factors, including efficient oxidative metabolism (reliance on aerobic respiration), a rich capillary supply, and efficient mechanisms for removing metabolic byproducts.
Metabolic Differences: Energy Production
The metabolic requirements and pathways for energy production also differ between cardiac and skeletal muscle.
1. Energy Sources: Skeletal muscle can utilize various energy sources, including anaerobic glycolysis (for short bursts of intense activity) and aerobic respiration (for sustained activity). Cardiac muscle primarily relies on aerobic respiration, using fatty acids as the main fuel source, supplemented by glucose and lactate. This reliance on aerobic respiration reflects the continuous need for ATP (adenosine triphosphate) to power the heart's constant contraction.
2. Oxidative Capacity: Cardiac muscle has a significantly higher oxidative capacity than skeletal muscle. This means it is better equipped to utilize oxygen for ATP production, contributing to its remarkable fatigue resistance. This high oxidative capacity is reflected in the rich capillary network surrounding cardiac muscle cells, ensuring an abundant supply of oxygen and nutrients.
Clinical Significance: Diseases and Conditions
Understanding the differences between cardiac and skeletal muscle is crucial in understanding various diseases and conditions affecting these tissues.
1. Cardiac Muscle Diseases: Conditions like heart failure, cardiomyopathies, and arrhythmias arise from dysfunction of cardiac muscle. These conditions can be caused by genetic factors, ischemic damage (lack of blood supply), infections, or other factors. The treatment strategies often involve medications aimed at modulating cardiac contractility, heart rate, or electrical conduction.
2. Skeletal Muscle Diseases: Skeletal muscle diseases, including muscular dystrophies, myasthenia gravis, and various inflammatory myopathies, reflect abnormalities in the structure or function of skeletal muscle. These conditions can lead to muscle weakness, fatigue, and pain. Treatment strategies vary depending on the specific disease and may involve supportive therapies, medications, or surgical interventions.
Summary Table: Key Differences
| Feature | Cardiac Muscle | Skeletal Muscle |
|---|---|---|
| Cell Shape | Branched, uninucleated | Long, cylindrical, multinucleated |
| Intercalated Discs | Present | Absent |
| Contraction | Involuntary, myogenic | Voluntary |
| Fatigue Resistance | High | Low |
| Primary Fuel | Fatty acids, glucose, lactate | Glucose, glycogen, fatty acids |
| Control | Autonomic nervous system, hormones | Somatic nervous system |
| T-tubules | Large, infrequent | Smaller, more frequent |
| SR development | Less developed than skeletal muscle | More developed than cardiac muscle |
Conclusion
The differences between cardiac and skeletal muscle highlight the remarkable adaptability of muscle tissue to perform diverse functions within the body. While both muscle types share the fundamental mechanism of sliding filaments for contraction, their structural organization, control mechanisms, metabolic pathways, and susceptibility to various diseases are significantly different. A thorough understanding of these differences is essential for appreciating the complex physiology of the human body and for diagnosing and treating a wide range of cardiovascular and musculoskeletal conditions. This detailed comparison provides a solid foundation for further exploration and deeper understanding of these vital muscle types. Remember to consult reliable sources such as textbooks and peer-reviewed articles for further in-depth study.
Latest Posts
Latest Posts
-
Cdl Combination Test Questions And Answers Pdf
Mar 18, 2025
-
Life Insurance Exam Questions And Answers Pdf
Mar 18, 2025
-
The Direct Carry Is Used To Transfer A Patient
Mar 18, 2025
-
The Emancipation Proclamation Of January 1 1863 Quizlet
Mar 18, 2025
-
These Cards Will Get You Drunk Quizlet
Mar 18, 2025
Related Post
Thank you for visiting our website which covers about Compared To Skeletal Muscle Cardiac Muscle Quizlet . We hope the information provided has been useful to you. Feel free to contact us if you have any questions or need further assistance. See you next time and don't miss to bookmark.
