Suggested Initial Dose Of Epinephrine Nrp 8th Edition
Breaking News Today
Mar 30, 2025 · 6 min read
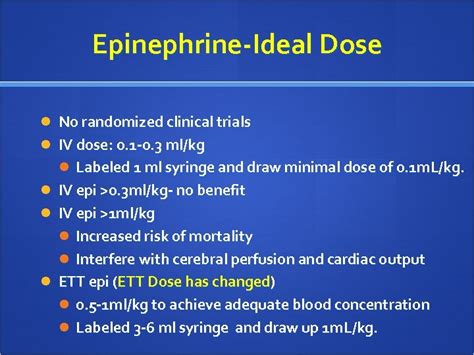
Table of Contents
Suggested Initial Dose of Epinephrine: NRP 8th Edition and Beyond
The 8th edition of the Neonatal Resuscitation Program (NRP) manual represents a significant update in the approach to neonatal resuscitation, particularly concerning the administration of epinephrine. Understanding the suggested initial dose and the nuances surrounding its use is crucial for healthcare professionals involved in neonatal care. This article delves deep into the NRP 8th edition guidelines on epinephrine administration, exploring the rationale behind the recommended dose, potential complications, and crucial considerations for its effective and safe application.
Understanding the Role of Epinephrine in Neonatal Resuscitation
Epinephrine, a potent sympathomimetic amine, plays a vital role in neonatal resuscitation by addressing two critical components of shock: poor perfusion and poor cardiac output. It acts by stimulating alpha and beta-adrenergic receptors, resulting in:
- Increased heart rate and contractility: Beta-1 stimulation enhances the force and rate of myocardial contractions, improving cardiac output.
- Increased peripheral vascular resistance: Alpha-1 stimulation constricts peripheral blood vessels, redirecting blood flow to vital organs like the brain and heart. This is particularly important in cases of hypovolemic shock.
- Bronchodilation: Beta-2 stimulation relaxes the smooth muscles of the bronchi, improving ventilation in cases of respiratory distress.
The NRP 8th Edition Recommendation: 0.01-0.03 mg/kg
The NRP 8th edition provides a clear recommendation for the initial dose of epinephrine in neonates requiring resuscitation: 0.01 to 0.03 mg/kg. This range reflects a shift in approach, emphasizing a more cautious and individualized titration of epinephrine based on the clinical presentation of the infant.
Why the Range?
The range of 0.01-0.03 mg/kg acknowledges the variability in individual responses to epinephrine. Factors such as gestational age, birth weight, and the underlying cause of the shock influence the optimal dose. A lower dose (0.01 mg/kg) might suffice for some infants, while others may require a higher dose (0.03 mg/kg) to achieve the desired physiological response.
The Importance of Accurate Calculation and Dilution
Precision in calculating and diluting the epinephrine dose is paramount. Incorrect dosing can have severe consequences. It's critical to meticulously calculate the exact volume required based on the infant's weight and the chosen concentration of epinephrine. Commonly used concentrations include 1:10,000 (0.1 mg/mL) and 1:1,000 (1 mg/mL). The chosen concentration will determine the volume to be administered.
Example: For a 2 kg infant, using a 1:10,000 solution, the 0.01 mg/kg dose would equate to 0.02 mg (2 kg x 0.01 mg/kg). This would require 0.2 mL of the 1:10,000 solution (0.02 mg / 0.1 mg/mL).
Route of Administration
The preferred route of administration for epinephrine in neonatal resuscitation remains intravascular, ideally via an umbilical venous catheter (UVC) or peripheral intravenous line. Endotracheal administration is considered an alternative route when intravenous access is not immediately available, although it is less effective and may cause a delay in achieving a therapeutic effect. The effectiveness of endotracheal epinephrine is significantly lower and absorption is unreliable.
When to Consider Epinephrine Administration
Epinephrine should not be routinely administered during neonatal resuscitation. Its use should be reserved for specific situations where there is clear evidence of persistent or recurring bradycardia unresponsive to initial resuscitation efforts including positive pressure ventilation and chest compressions. These situations include:
- Persistent bradycardia (<60 bpm) despite adequate ventilation and chest compressions: This indicates inadequate cardiac output and perfusion.
- Persistent asystole or pulseless electrical activity (PEA): Epinephrine is crucial in these life-threatening situations.
- Shock: Signs of shock such as poor perfusion (mottling, acrocyanosis, weak pulses), hypotension, and metabolic acidosis warrant epinephrine administration.
Monitoring Response and Subsequent Doses
After administering epinephrine, close monitoring of the infant's heart rate, blood pressure, and perfusion is vital. The response to the initial dose can vary widely. Some infants will show a rapid and sustained improvement, while others may require further doses. Subsequent doses should only be administered if there is no significant improvement in the infant's condition. The NRP 8th edition does not provide a specific recommendation for repeat dosing, emphasizing the importance of clinical judgment and titration based on the infant's response.
Potential Complications of Epinephrine Administration
While epinephrine is crucial in life-threatening situations, it's essential to be aware of potential adverse effects:
- Hypertension: Epinephrine can cause a significant increase in blood pressure, potentially leading to complications in vulnerable infants. Close monitoring of blood pressure is essential.
- Arrhythmias: In rare cases, epinephrine can trigger or worsen arrhythmias.
- Tissue necrosis: Extravasation of epinephrine during intravenous administration can cause local tissue damage.
- Metabolic acidosis: While epinephrine may improve perfusion, it can exacerbate metabolic acidosis in certain scenarios.
Beyond the Initial Dose: A Holistic Approach
The NRP 8th edition's emphasis on the 0.01-0.03 mg/kg range underscores a move toward a more nuanced approach to epinephrine administration. It is not a "one-size-fits-all" solution. The optimal dose is highly dependent on various factors. The focus should always be on the underlying cause of the infant's distress. Effective resuscitation requires addressing the underlying cause of the shock or bradycardia – whether it is hypovolemia, hypoxia, or acidosis. Providing adequate ventilation, chest compressions, and addressing potential underlying causes are equally critical to a successful resuscitation outcome.
Integrating Other Resuscitation Techniques
Epinephrine is only one component of neonatal resuscitation. Its effective use must be integrated with other crucial resuscitation techniques, including:
- Adequate ventilation: Providing positive pressure ventilation with the appropriate rate and tidal volume is critical.
- Effective chest compressions: High-quality chest compressions are vital in maintaining perfusion when the heart is not adequately pumping blood.
- Volume expansion: In cases of hypovolemic shock, fluid resuscitation is essential.
- Correction of acidosis: If metabolic acidosis is present, appropriate interventions should be implemented.
Continuous Learning and Refinement
The field of neonatal resuscitation continues to evolve. Healthcare professionals involved in neonatal care must stay updated with the latest guidelines and advancements in resuscitation techniques. Regular participation in NRP courses and continuous review of best practices are essential to ensure the best possible outcomes for infants requiring resuscitation.
Conclusion: A Cautious and Individualized Approach
The NRP 8th edition's suggested initial dose of epinephrine, ranging from 0.01 to 0.03 mg/kg, reflects a thoughtful and evidence-based approach to neonatal resuscitation. It emphasizes the importance of a cautious and individualized strategy, tailored to the unique needs of each infant. While epinephrine plays a crucial role in addressing profound bradycardia and shock, its effective use requires a thorough understanding of its mechanism of action, potential complications, and its integration within a comprehensive resuscitation strategy. Continuous learning and a dedication to providing optimal care are key elements in ensuring positive outcomes for newborns. The success of resuscitation hinges on a multifaceted approach that includes prompt recognition of the need for intervention, accurate assessment of the infant's condition, precise medication administration, and continuous monitoring of the infant's response. Effective teamwork and adherence to established protocols remain crucial to achieving successful neonatal resuscitation.
Latest Posts
Latest Posts
-
What Step Should Be Taken Next To Securely Telework
Apr 01, 2025
-
Apprentices Typically Receive A Pay Increase After Each
Apr 01, 2025
-
The Presidents Challenge Program Is A Fitness Evaluation Designed For
Apr 01, 2025
-
Amoeba Sisters Video Recap Answers Dna Replication
Apr 01, 2025
-
Which Of These Is Underconsumed In The United States
Apr 01, 2025
Related Post
Thank you for visiting our website which covers about Suggested Initial Dose Of Epinephrine Nrp 8th Edition . We hope the information provided has been useful to you. Feel free to contact us if you have any questions or need further assistance. See you next time and don't miss to bookmark.
